
- Optic neuritis. (T/F?)
- Lhermitte’s sign. (T/F?)
- Fatigue. (T/F?)
- Hypoesthesias. (T/F?)
- Internuclear ophthalmoplegia. (T/F?)
- Trigeminal neuralgia. (T/F?)
9. Etiology of MS
- The concordance rate for a clinical diagnosis of the disease in identical twins is about 30%. (T/F?)
- Adoptive children, when raised from infancy in families with a high prevalence of the disease, have three times greater incidence of the disease then the general population. (T/F?)
- It is associated with both MHC and HLA antigens. (T/F?)
- Low levels of vitamin D have not been associated with an increased risk for the disease. (T/F?)
- Smoking is an independent risk factor. (T/F?)
- History of infectious mononucleosis, as opposed to the asymptomatic EBV infection, does not implicate greater risk for the disease. (T/F?)
8. CSF in MS:
- Opening pressure: elevated. (T/F?)
- Cell count: increased (5–50 lymphocytes/mm 3 ) in two-thirds of patients during an acute attack. (T/F?)
- Protein: can be mildly elevated, up to 100 mg/dl. (T/F?)
- Oligoclonal IgG bands: present in more then 90% patients. (T/F?)
- IgG index : elevated in about 90% of patients with clinically definite MS. (T/F?)
- Oligoclonal IgG bands are specific for this disease. (T/F?)
7. Internuclear ophthalmoplegia:
- Results in double vision, due to lesion of the medial longitudinal fasciculus (MLF), which connects the nuclei of oculomotor and abducens nerves. (T/F?)
- Is always unilateral. (T/F?)
- Diplopia is elicited with the gaze to the opposite side of the affected eye. (T/F?)
- Affected eye shows impairment ( slower rate or failure ) of adduction. (T/F?)
- Contralateral (not affected) eye shows vertical nystagmus with abduction. (T/F?)
- If the left eye is affected, the patient will have diplopia when looking to the left. (T/F?)
- With rostral MLF lesions, near the oculomotor nucleus, convergence of the eyes may be impaired. (T/F?)
6. Signs and symptoms of optic neuritis
- Reduced visual acuity. (T/F?)
- Dulling of color vision in the affected eye. (T/F?)
- Pain around the eye that is not affected by eye movement or touching the eye. (T/F?)
- Transient worsening of vision with decrease of body temperature. (T/F?)
- Ophthalmoscopy findings are frequently normal. (T/F?)
- Are frequent initial symptoms of multiple sclerosis. (T/F)
5. Trigeminal nerve
- Is the largest cranial nerve. (T/F?)
- Is both motor and sensory nerve. (T/F?)
- Has three major branches: the ophthalmic nerve, the maxillary nerve, and the mandibular nerve. (T/F?)
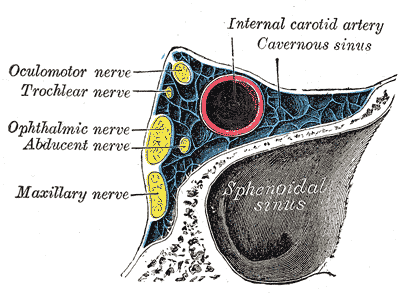
- One of its branches, mandibular nerve comes close to the internal carotid artery in the cavernous sinus. (T/F?)
- Its motor nucleus supplies the muscles of mastication. (T/F)
- Maxillary and mandibular nerve have sensory and motor functions. (T/F?)



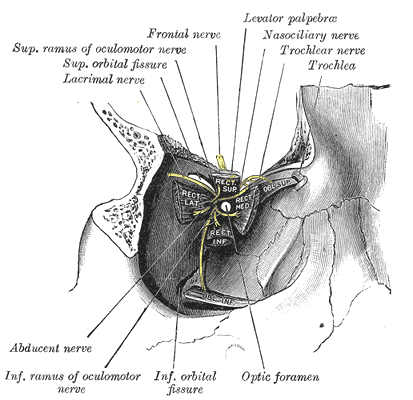
4. Oculomotor nerve
- Is the third cranial nerve. (T/F?)
- Has two nuclei: oculomotor nucleus and the Edinger-Westphal nucleus. (T/F)
- Runs in the lateral wall of the cavernous sinus. (T/F?)
- Enters orbit through the inferior orbital fissure. (T/F?)
- Its upper division supplies the superior rectus and the superior oblique muscles. (T/F?)
- Its inferior branch innervates medial rectus, inferior rectus and inferior oblique muscles. (T/F?)
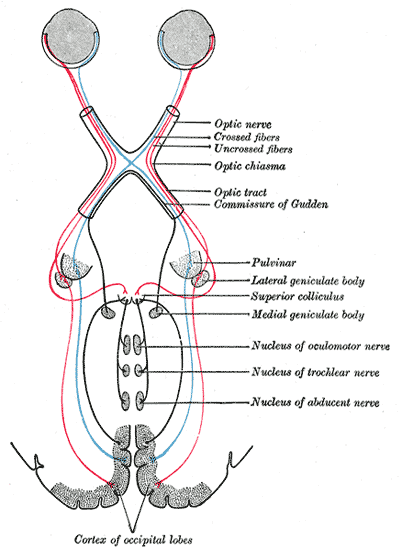
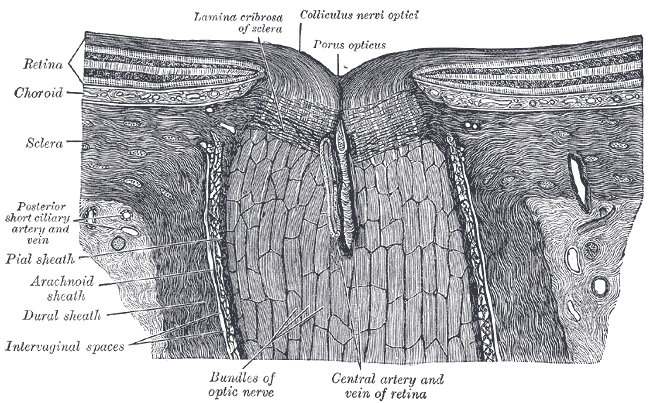
3. Optic nerve
- Is also known as the second cranial nerve. (T/F?)
- Is wrapped around with Schwann cells. (T/F?)
- Is covered with all three meningeal layers. (T/F?)
- Leaves the orbit through superior orbital fissure. (T/F?)
- Is not affected with Guillain–Barré syndrome. (T/F?)
- Some of its axons terminate in the pretectal nuclei. (T/F?)
{kind=link}
{kind=link}