- The trochlear nerve innervates only one muscle, the superior oblique muscle of the eye. (T/F?)
- The superior oblique muscle abducts, depresses and externaly rotates the eye. (T/F?)
- An injury to the trochlear nerve causes horizontal diplopia. (T/F?)
- An injury to the trochlear nucleus will result in symptoms in the eye on the same side. (T/F?)
- An injury to the trochlear nerve, after it exits the mesencephalon, will result in symptoms in the eye on the same side. (T/F?)
- An eye affected with the trochlear nerve palsy is positioned upwards relative to the unaffected eye. (T/F?)
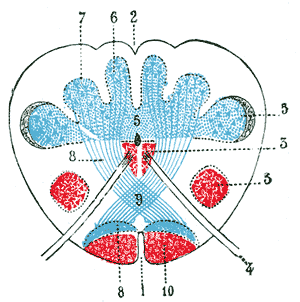
90. Transverse section through the sensory decussation (Gray714)
89. The tarts
The cranial nerves passing through the superior orbital fissure in order from top to bottom:
- Lacrimal nerve. (T/F?)
- Frontal nerve. /T/F?)
- Trochlear nerve. (T/F?)
- Superior branch of the oculomotor nerve. (T/F?)
- Nasocilliary nerve. (T/F?)
- Abducens nerve. (T/F?)
- Inferior branch of the oculomotor nerve. (T/F?)
88. Entry and exit points of cranial nerves, arteries and veins (II)
- Anterior ethmoidal artery: Foramen cecum. (T/F?)
- Ophtalmic artery: Superior orbital fissure. (T/F?)
- Ophtalmic nerve: Superior orbital fissure. (T/F?)
- Superior ophtalmic vein: Superior orbital fissure. (T/F?)
- Maxillary nerve: Foramen rotundum. (T/F?)
- Glossopharyngeal nerve: Jugular foramen. (T/F?)
87. Corpus callosum
- On the superior surface of the corpus callosum lies a thin layer of grey matter. (T/F?)
- Septum pellucidum is situated beneath the splenium of the corpus callosum. (T/F?)
- The forceps major connects parts of the frontal lobes and its fibers pass through the genu of the corpus callosum. (T/F?)
- The occipital lobes are connected through the splenium of the corpus callosum. (T/F?)
- The temporal lobes are connected by the anterior commissure. (T/F?)
- The kangaroos don’t have a corpus callosum. (T/F?)
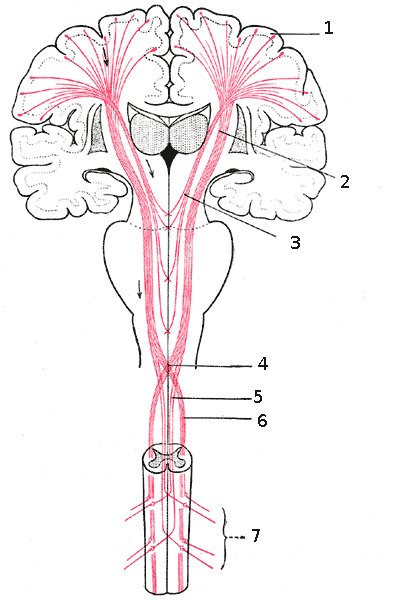
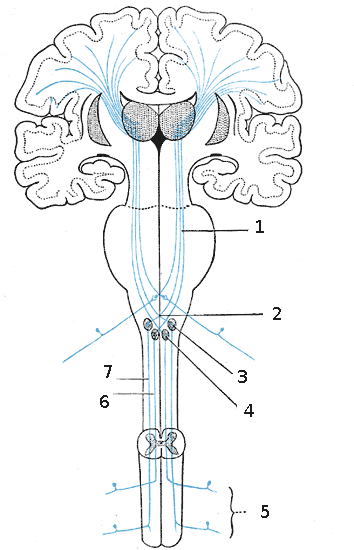
85. Sensory decussation (Gray759)
84. Decussations [X]
- The lateral corticospinal tracts decussate in the pyramids of the lower medulla. (T/F?)
- The posterior spinocerebellar tracts decussate one to two levels above their entry points in the spinal cord. (T/F?)
- The fibers of the anterior corticospinal tract decussate in the pyramids of the lower medulla. (T/F?)
- The lateral spinothalamic tracts decussate in the lower medulla. (T/F?)
- The anterior spinocerebellar tracts do not decussate. (T/F?)
- The dorsal column tracts decussate in the lower medulla. (T/F?)
83. Spinal nerves and anatomical landmarks
- Nipple – T4. (T/F?)
- Umbilicus – T10. (T/F?)
- Thumb – C5. (T/F?)
- Medial malleolus – L4. (T/F?)
- Little finger – C7. (T/F?)
- Middle finger – C6. (T/F?)
81. One and a half syndrome
- The one and a half syndrome is characterized by a conjugate horizontal gaze palsy in one direction and an impairment of the abduction of the eyes in the other. (T/F?)
- Horizontal gaze palsy is seen on looking away from the side of the lesion. (T/F?)
- The ipsilateral eye has no horizontal movement. (T/F?)
- The most common cause of the one-and-a-half syndrome in the young people is Miller-Fisher syndrome. (T/F?)
- The most common cause of the one-and-a-half syndrome in older people is multiple sclerosis. (T/F?)
- When the lesion that causes a damage to PPRF or abducens nucleus and medial longitudinal fasciculus, also affects the facial nerve, we can talk about an eight-and-a-half syndrome. (T/F?)